A fall, a fractured ankle, and what should have been a predictable recovery instead became a prolonged struggle with pain — and a legal lesson on how medical records can make or break a defence.
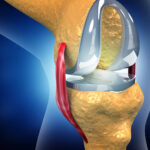
The patient was admitted with an ankle injury after a fall and underwent surgery for fixation. Hospital records showed that the treating team was aware of multiple fractures around the ankle joint. She was discharged with assurances of recovery and followed up with physiotherapy as advised. Yet weeks after the cast was removed, she continued to experience severe pain, swelling, and difficulty bearing weight.
Seeking other opinions, she was told that one fracture had never been properly addressed. This formed the basis of her negligence complaint.
The hospital denied any lapse. It argued that the surgery was done according to accepted orthopaedic protocol, that post-operative X-rays showed proper alignment, and that the patient had improved with physiotherapy. Crucially, it relied on a typed discharge summary to argue that only certain fractures existed — and that others were either undisplaced or ligament-related and adequately treated with casting.
But the court focused on something far more basic: the hospital’s own paperwork.
On record were two versions of the discharge summary — one handwritten and one typed. Instead of matching, they contradicted each other on a vital point. The handwritten notes clearly recorded a fracture that was completely missing from the typed version. Since typed summaries are prepared from handwritten notes, the inconsistency raised an uncomfortable inference: the fracture was known, but not treated.
The hospital attempted to explain this away by saying the handwritten note was prepared by an intern and that the typed summary was the “final” document. The Commission rejected this outright, observing that a hospital cannot escape responsibility by blaming interns for errors in documents as critical as discharge summaries.
What further weakened the defence was the hospital’s own pleadings. In one breath, it claimed the fracture was not evident; in another, it stated that the same fracture was treated conservatively. The court found this contradiction impossible to reconcile.
Even an expert medical board opinion favouring the hospital did not rescue the case. The Commission noted that expert opinions are advisory, not binding, and may be disregarded when they overlook key records or fail to address the real controversy. Independent orthopaedic opinions obtained by the patient, which specifically identified the untreated fracture, were found more persuasive.
The appeal was dismissed. The finding of negligence and the compensation awarded by the District Commission were upheld.
IML Insight
This case is a reminder that medical negligence is often proved not in the operation theatre, but on paper. Discharge summaries are not clerical formalities — they are legal documents. When records contradict each other, courts are entitled to presume that something essential was missed. For hospitals, internal consistency, supervision of junior staff, and record verification are not administrative tasks — they are risk controls.